
Bilingual
En/Fa
Geographical Research is Published in both Persian and English Full-text.
Volume 39, Issue 2 (2024)
GeoRes 2024, 39(2): 215-223 |
Back to browse issues page
Article Type:
Subject:






Research code: 1612
History
Received: 2024/05/5 | Accepted: 2024/06/26 | Published: 2024/07/10
Received: 2024/05/5 | Accepted: 2024/06/26 | Published: 2024/07/10
How to cite this article
Alidadi S, Dehghan H, Rezaei N. The Role of Cultural Factors in the Development of Medical Tourism in Primary Health Tourism Centers in Iran. GeoRes 2024; 39 (2) :215-223
URL: http://georesearch.ir/article-1-1612-en.html
URL: http://georesearch.ir/article-1-1612-en.html
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



Rights and permissions
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:

1- Department of Sociology, Economics and Development, Faculty of Humanities, North Tehran Branch, Islamic Azad University, Tehran, Iran
2- Department of Social Sciences, Faculty of Humanities, North Tehran Branch, Islamic Azad University, Tehran, Iran
3- Tourism Research Group, Research Institute of Cultural Heritage and Tourism, Tehran, Iran
2- Department of Social Sciences, Faculty of Humanities, North Tehran Branch, Islamic Azad University, Tehran, Iran
3- Tourism Research Group, Research Institute of Cultural Heritage and Tourism, Tehran, Iran
Full-Text (HTML) (401 Views)
Background
Tourism is a major global industry that plays a vital role in countries' economic and social development. Health tourism, as a growing branch, focuses on medical services and well-being and has become a global industry. Technological advances, cultural shifts, and intercultural interactions have fueled its growth. Iran, with its cultural, geographical, and infrastructural strengths, has high potential for developing medical tourism.
Previous Studies
Various studies have examined the factors influencing medical tourism. For example, Smith & Forgione (2007) identify hospital accreditation, and Adams & Wright (1991) have highlighted geographical distance as important factors in choosing a medical destination. Glinos et al. (2010) emphasizes the role of cultural familiarity in patients’ decision-making. Mosadeghrad & Sadeghi (2021) have stressed that cultural factors play a key role in the process of selecting the destination country. Bakhtiarivafa (2020) regardes the development of medical infrastructure as a driver for expanding health tourism. Ramezani Hajimahaleh (2019) considers Iran to have high potential for attracting health tourists due to its favorable cultural position. Mamramezani (2017) points to the importance of components such as trust, professional workforce, service diversity, and cultural programs in patient satisfaction. Additionally, Baycan (2013) has reported a positive correlation between service quality and patient loyalty, while Esiyok et al. (2017) have demonstrated that cultural distance directly affects the choice of medical tourism destination.
Aim(s)
This study aims to examine the cultural factors influencing the development of health tourism in major health tourism centers in Iran, with the goal of identifying these factors to improve and refine planning and policymaking by the relevant stakeholders.
Research Type
The present study was a fundamental and applied research and, in terms of data collection and analysis methods, it was descriptive and survey-based.
Research Society, Place and Time
The statistical population of this study included all foreign medical tourists in five cities of Tehran, Shiraz, Tabriz, Mashhad, and Ahvaz. These five provinces were purposefully selected as the main centers providing health tourism services in the country. The geographical scope of the research was limited to the aforementioned cities in Iran, and data collection took place between the years 2021 and 2023.
Sampling Method and Number
In this study, due to the unlimited size of the statistical population, a simple random sampling method was used. First, five main provinces providing health tourism services (Tehran, Shiraz, Tabriz, Mashhad, and Ahvaz) were purposefully selected. Then, one hospital from each city was chosen using cluster sampling. Subsequently, foreign medical tourists visiting these hospitals were selected by simple random sampling based on the type of services received (medical, cosmetic, etc.). The sample size was determined to be 384 individuals using Morgan’s table.
Used Devices & Materials
In this study, the main data collection tool was a researcher-designed questionnaire consisting of 112 closed-ended questions. Of these, 64 questions were structured as Likert-scale items with five options (ranging from very high to very low), and 46 questions were designed as two-option items. The questionnaire was divided into two sections including the demographic questions (such as age, gender, nationality, education, etc.), and the second contained indicators and items related to culture and health tourism. For data analysis, SPSS version 22 and LISREL version 12 software were used. Additionally, Cronbach’s alpha coefficient was employed to assess the reliability of the questionnaire, and face validity was evaluated through the opinions of university experts and specialists in the field.
Findings by Text
The findings of this study showed that more than half of the medical tourists surveyed were women, with the majority holding a diploma-level education (Table 1). In terms of nationality, Iraqi tourists were the most frequent. The normality test confirmed that the study variables followed a normal distribution, allowing the use of Pearson correlation for relationship analysis (Table 2). Results indicated a significant positive relationship between material culture and the development of medical tourism, where a one-unit increase in material culture corresponded to a 0.374 increase in medical tourism development. Among the components of material culture, cultural heritage sites were the most influential factor. Additionally, spiritual culture showed a stronger correlation with medical tourism (correlation coefficient of 0.623), with health resorts playing the most prominent role in this dimension (Table 2).
Table 1. Demographic characteristics
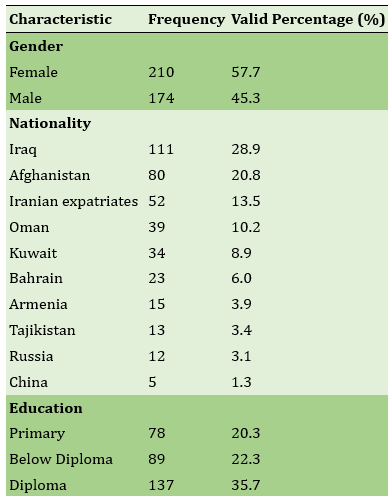
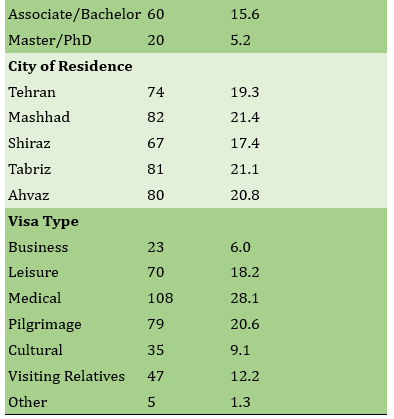
Table 2. Examining the effect of the independent contextual parameter gender on spiritual culture

Demographic variable analysis revealed that gender and age had no significant relationship with spiritual culture, but higher education was associated with a greater inclination toward spiritual culture (Table 2). Conversely, both gender and age influenced material culture, with women and older individuals showing a stronger tendency toward material cultural components, while education had no significant effect on this dimension (Table 3). Overall, the path analysis model demonstrated that spiritual culture (path coefficient of 0.92) and, subsequently, material culture (path coefficient of 0.73) had the greatest impact on medical tourism development, highlighting the fundamental role of cultural factors in shaping and advancing this type of tourism.
Table 3. Examining the relationship between the independent contextual parameter gender and material culture

Main Comparisons to Similar Studies
This study’s findings on cultural factors affecting medical tourism align with previous research. Ramezani Hajimahaleh (2019) highlights Iran’s cultural strengths and strategic location attracting Muslim medical tourists. Kharazmi et al. (2016) also emphasize cultural factors’ impact on foreign tourists. Lee and Spisto (2007) found out cultural familiarity and language ease increase destination appeal, while Connell (2013) notes shared cultural-religious backgrounds reduce cultural shock, boosting medical tourism. Smith and Puczko (2014) stress that rich cultural heritage and strong ties to tourists attract more medical travelers.
Mamramezani (2017) confirms the importance of cultural programs and technology in health tourism development, supporting this study’s findings on material and spiritual culture. Gender differences with women showing stronger cultural preferences agree with Duffy et al. (2001) and Ehrbeck et al. (2008). Baycan (2013) and Esiyok et al. (2017) explore related cultural distance effects. Overall, the study reinforces culture’s key role in medical tourism growth, despite challenges like COVID-19 affecting data collection.
Suggestions
To develop medical tourism, Iran should leverage its cultural, religious, and natural attractions and improve hospitality. Strengthening cooperation between sectors through specialized working groups and enhancing institutional collaboration is essential. Establishing a dedicated national body to coordinate policies and promote medical tourism internationally is also recommend
Conclusion
There is a significant relationship between material culture and spiritual culture with the development of medical tourism. While gender and age significantly affect material culture, women and older individuals show a greater tendency toward material cultural factors. Only education has a significant impact on spiritual culture.
Acknowledgments: None reported by the authors.
Ethical Permission: None reported by the authors.
Conflict of Interest: This article is extracted from the PhD thesis of Simin Behbahani in Islamic Azad University of Tehran.
Authors’ Contributions: Alidadi S M (First author), Main Researcher (50%); Dehghan H (Second author), Methodologist (25%); Rezaei N (Third author), Discussion Writer/Statistical Analyst (25%).
Funding: None reported by the authors.
Tourism is a major global industry that plays a vital role in countries' economic and social development. Health tourism, as a growing branch, focuses on medical services and well-being and has become a global industry. Technological advances, cultural shifts, and intercultural interactions have fueled its growth. Iran, with its cultural, geographical, and infrastructural strengths, has high potential for developing medical tourism.
Previous Studies
Various studies have examined the factors influencing medical tourism. For example, Smith & Forgione (2007) identify hospital accreditation, and Adams & Wright (1991) have highlighted geographical distance as important factors in choosing a medical destination. Glinos et al. (2010) emphasizes the role of cultural familiarity in patients’ decision-making. Mosadeghrad & Sadeghi (2021) have stressed that cultural factors play a key role in the process of selecting the destination country. Bakhtiarivafa (2020) regardes the development of medical infrastructure as a driver for expanding health tourism. Ramezani Hajimahaleh (2019) considers Iran to have high potential for attracting health tourists due to its favorable cultural position. Mamramezani (2017) points to the importance of components such as trust, professional workforce, service diversity, and cultural programs in patient satisfaction. Additionally, Baycan (2013) has reported a positive correlation between service quality and patient loyalty, while Esiyok et al. (2017) have demonstrated that cultural distance directly affects the choice of medical tourism destination.
Aim(s)
This study aims to examine the cultural factors influencing the development of health tourism in major health tourism centers in Iran, with the goal of identifying these factors to improve and refine planning and policymaking by the relevant stakeholders.
Research Type
The present study was a fundamental and applied research and, in terms of data collection and analysis methods, it was descriptive and survey-based.
Research Society, Place and Time
The statistical population of this study included all foreign medical tourists in five cities of Tehran, Shiraz, Tabriz, Mashhad, and Ahvaz. These five provinces were purposefully selected as the main centers providing health tourism services in the country. The geographical scope of the research was limited to the aforementioned cities in Iran, and data collection took place between the years 2021 and 2023.
Sampling Method and Number
In this study, due to the unlimited size of the statistical population, a simple random sampling method was used. First, five main provinces providing health tourism services (Tehran, Shiraz, Tabriz, Mashhad, and Ahvaz) were purposefully selected. Then, one hospital from each city was chosen using cluster sampling. Subsequently, foreign medical tourists visiting these hospitals were selected by simple random sampling based on the type of services received (medical, cosmetic, etc.). The sample size was determined to be 384 individuals using Morgan’s table.
Used Devices & Materials
In this study, the main data collection tool was a researcher-designed questionnaire consisting of 112 closed-ended questions. Of these, 64 questions were structured as Likert-scale items with five options (ranging from very high to very low), and 46 questions were designed as two-option items. The questionnaire was divided into two sections including the demographic questions (such as age, gender, nationality, education, etc.), and the second contained indicators and items related to culture and health tourism. For data analysis, SPSS version 22 and LISREL version 12 software were used. Additionally, Cronbach’s alpha coefficient was employed to assess the reliability of the questionnaire, and face validity was evaluated through the opinions of university experts and specialists in the field.
Findings by Text
The findings of this study showed that more than half of the medical tourists surveyed were women, with the majority holding a diploma-level education (Table 1). In terms of nationality, Iraqi tourists were the most frequent. The normality test confirmed that the study variables followed a normal distribution, allowing the use of Pearson correlation for relationship analysis (Table 2). Results indicated a significant positive relationship between material culture and the development of medical tourism, where a one-unit increase in material culture corresponded to a 0.374 increase in medical tourism development. Among the components of material culture, cultural heritage sites were the most influential factor. Additionally, spiritual culture showed a stronger correlation with medical tourism (correlation coefficient of 0.623), with health resorts playing the most prominent role in this dimension (Table 2).
Table 1. Demographic characteristics
Table 2. Examining the effect of the independent contextual parameter gender on spiritual culture
Demographic variable analysis revealed that gender and age had no significant relationship with spiritual culture, but higher education was associated with a greater inclination toward spiritual culture (Table 2). Conversely, both gender and age influenced material culture, with women and older individuals showing a stronger tendency toward material cultural components, while education had no significant effect on this dimension (Table 3). Overall, the path analysis model demonstrated that spiritual culture (path coefficient of 0.92) and, subsequently, material culture (path coefficient of 0.73) had the greatest impact on medical tourism development, highlighting the fundamental role of cultural factors in shaping and advancing this type of tourism.
Table 3. Examining the relationship between the independent contextual parameter gender and material culture
Main Comparisons to Similar Studies
This study’s findings on cultural factors affecting medical tourism align with previous research. Ramezani Hajimahaleh (2019) highlights Iran’s cultural strengths and strategic location attracting Muslim medical tourists. Kharazmi et al. (2016) also emphasize cultural factors’ impact on foreign tourists. Lee and Spisto (2007) found out cultural familiarity and language ease increase destination appeal, while Connell (2013) notes shared cultural-religious backgrounds reduce cultural shock, boosting medical tourism. Smith and Puczko (2014) stress that rich cultural heritage and strong ties to tourists attract more medical travelers.
Mamramezani (2017) confirms the importance of cultural programs and technology in health tourism development, supporting this study’s findings on material and spiritual culture. Gender differences with women showing stronger cultural preferences agree with Duffy et al. (2001) and Ehrbeck et al. (2008). Baycan (2013) and Esiyok et al. (2017) explore related cultural distance effects. Overall, the study reinforces culture’s key role in medical tourism growth, despite challenges like COVID-19 affecting data collection.
Suggestions
To develop medical tourism, Iran should leverage its cultural, religious, and natural attractions and improve hospitality. Strengthening cooperation between sectors through specialized working groups and enhancing institutional collaboration is essential. Establishing a dedicated national body to coordinate policies and promote medical tourism internationally is also recommend
Conclusion
There is a significant relationship between material culture and spiritual culture with the development of medical tourism. While gender and age significantly affect material culture, women and older individuals show a greater tendency toward material cultural factors. Only education has a significant impact on spiritual culture.
Acknowledgments: None reported by the authors.
Ethical Permission: None reported by the authors.
Conflict of Interest: This article is extracted from the PhD thesis of Simin Behbahani in Islamic Azad University of Tehran.
Authors’ Contributions: Alidadi S M (First author), Main Researcher (50%); Dehghan H (Second author), Methodologist (25%); Rezaei N (Third author), Discussion Writer/Statistical Analyst (25%).
Funding: None reported by the authors.
References
1. Adams EK, Wright GE (1991). Hospital choice of medicare beneficiaries in a rural market: Why not the closest?. The Journal of Rural Health. 7(2):134-152. [Link] [DOI:10.1111/j.1748-0361.1991.tb00715.x]
2. Alizadeh S, Chavan M (2016). Cultural competence dimensions and outcomes: A systematic review of the literature. Health and Social Care in the Community. 24(6):117-130. [Link] [DOI:10.1111/hsc.12293]
3. Bakhtiarivafa P (2020). Design of the space provided with Health Tourism Promotion Approach (case study of Hamedan city). [Dissertation]. Hamedan: Institute of Higher Education, Hamedan Branch of ACECR. [Persian] [Link]
4. Bartzis G, Kaitelidou D, Bistaraki A, Konstantakopoulou O (2020). Factors affecting medical tourism destination selection in Greece. Studies in Health Technology and Informatics. 272:314-317. [Link]
5. Baycan T (2013). Knowledge commercialization and valorization in regional economic development. Cheltenham: Edward Elgar Publishing. [Link] [DOI:10.4337/9781781004074]
6. Chambers N, Cifter A (2022). Working capital management and firm performance in the hospitality and tourism industry. International Journal of Hospitality Management. 102:103144. [Link] [DOI:10.1016/j.ijhm.2022.103144]
7. Chang L, Beise-Zee R (2013). Consumer perception of healthfulness and appraisal of health-promoting tourist destinations. Tourism Review. 68(1):34-47. [Link] [DOI:10.1108/16605371311310066]
8. Connell J (2013). Contemporary medical tourism: Conceptualisation, culture and commodification. Tourism Management. 34:1-13. [Link] [DOI:10.1016/j.tourman.2012.05.009]
9. Duffy LN, Kline C, Mowatt R, Chancellor C (2001). Women's health and wellness. New York: Sage Publications. [Link]
10. Ehrbeck T, Guevara C, Mango PD (2008). Mapping the market for medical travel. Seattle: The McKinsey Quarterly. [Link]
11. Esiyok B, Çakar M, Kurtulmuşoğlu FB (2017). The effect of cultural distance on medical tourism. Journal of Destination Marketing & Management. 6(1):66-75. [Link] [DOI:10.1016/j.jdmm.2016.03.001]
12. Geitona M, Sarantopoulos J (2015). Medical tourism: Investment in health and economy. Athens: Papazisis. [Link]
13. Ghasemi Yalghouzaghaj A, Assadzadeh A, Imani Khoshkhoo MH, Jabbarzadeh Y (2018). The impact of medical tourism motivational factors on behavioral intentions of tourists: The mediating role of perceptual factors and satisfaction. Journal of Tourism Planning and Development. 7(24):59-81. [Persian] [Link]
14. Giddens A (1985). The nation-state and violence. Berkeley: University of California Press. [Link]
15. Glinos IA, Baeten R, Helble M, Maarse H (2010). A typology of cross-border patient mobility. Health and Place. 16(6):1145-1155. [Link] [DOI:10.1016/j.healthplace.2010.08.001]
16. Helmy EM, Travers R (2009). Towards the development of Egyptian medical tourism sector. Anatolia. 20(2):419-439. [Link] [DOI:10.1080/13032917.2009.10518918]
17. Herrick DM (2007). Medical tourism: Global competition in health care. Texas: National Center for Policy Analysis. No. 304. [Link]
18. Horowitz MD, Rosensweig JA, Jones CA (2007). Medical tourism: Globalization of the healthcare marketplace. Medscape General Medicine. 9(4):33-42. [Link]
19. Izadi H (2002). A perspective on the global impact of Islamic cultures and civilizations. MESBAH. 10(37):57-76. [Persian] [Link]
20. Kharazmi A, Rahnama MR, Javan J, Shokouhi MA (2016). Factors affecting the promotion of health tourism; Comparative view of foreign tourists and domestic managers. Journal of North Khorasan. 8(3):405-416. [Persian] [Link] [DOI:10.18869/acadpub.jnkums.8.3.405]
21. Lee C, Spisto M (2007). Medical tourism, the future of health services. Proceedings of the 12th International Conference on ISO 9000 and TQM. Taiwan: National Chin-Yi University of Technology. p. 1-7. [Link]
22. Mosadeghrad AM, Sadeghi M (2021). Medical tourism: Reasons for choosing Iran. PAYESH. 20(2):145-166. [Persian] [Link] [DOI:10.52547/payesh.20.2.145]
23. Mamramezani K (2017). Evaluation of health tourism as an approach in the development of border areas, case study: Kurdistan province [Dissertation]. Tehran: Tehran University [Persian] [Link]
24. Ramezani Hajimahaleh A (2019). Spatial analysis of health tourism in urban areas (case study: public hospitals in Tehran) [Dissertation]. Tehran: Shahid Beheshti University. [Persian] [Link]
25. Rokni L, Park SH, Avci T (2019). Improving medical tourism services through human behaviour and cultural competence. Iranian Journal of Public Health. 48(11):1988-1996. [Link] [DOI:10.18502/ijph.v48i11.3517]
26. Salasi M (2000). World of Iran and Iran's world. Tehran: Markaz Publications. [Persian] [Link]
27. Sandberg D (2017). Medical tourism: An emerging global healthcare industry. International Journal of Healthcare Management. 10(4):281-288. [Link] [DOI:10.1080/20479700.2017.1296213]
28. Smith M, Puczko L (2014). Health, tourism and hospitality: Spas, wellness and medical travel. London: Routledge. [Link] [DOI:10.4324/9780203083772]
29. Smith PC, Forgione DA (2007). Global outsourcing of healthcare: A medical tourism decision model. Journal of Information Technology Case and Application Research. 9(3):19-30. [Link] [DOI:10.1080/15228053.2007.10856117]
30. Theofanides F, Papanikolaou V (2012). Exploring and exploiting medical tourism opportunities in Greece. Proceedings of the 2nd Advances in Hospitality and Tourism Marketing & Management Conference, Corfu, Greece. [Link]
31. Traouda V, Mpogiatzidis P (2021). Dialysis and medical tourism. Investigating patients' perceptions in Greece. International Journal of Human Rights in Healthcare. 14(5):411-425. [Link] [DOI:10.1108/IJHRH-10-2020-0090]
32. Velissariou E, Triantafyllos T (2014). Tourism and medical services. The case of elective medical tourism in Northern Greece. Proceedings of the 2nd International Conference of Tourism, Hospitality and Recreation. Poland: EJTHR. [Link]
33. Yang JY, Paek S, Kim T, Lee TH (2015). Health tourism: Needs for healing experience and intentions for transformation in wellness resorts in Korea. International Journal of Contemporary Hospitality Management. 27(8):1881-1904. [Link] [DOI:10.1108/IJCHM-11-2013-0505]
34. Zargham Boroujeni H, Sedaghat M (2018). A process model for sustainable tourism development of Islamic Republic of Iran (a Grounded Theory Model based on five-year economic, social and cultural plans of Iran), Journal of Tourism and Development. 7(3):25-73. [Persian] [Link]